When caregiving is stereotyped as ‘women’s work’, the physical and emotional labour involved disproportionately affects women. The Covid-19 pandemic magnified these issues. Women in these roles also end up feeling morally distressed, as the load of their responsibilities forces them to sacrifice the level of care they want to provide. Not only that, this is detrimental to the entire care economy and nation’s well being.
Text: Foong Li Mei
Illustration: Faizati Mohd Ali
Text: Foong Li Mei
Illustration: Faizati Mohd Ali
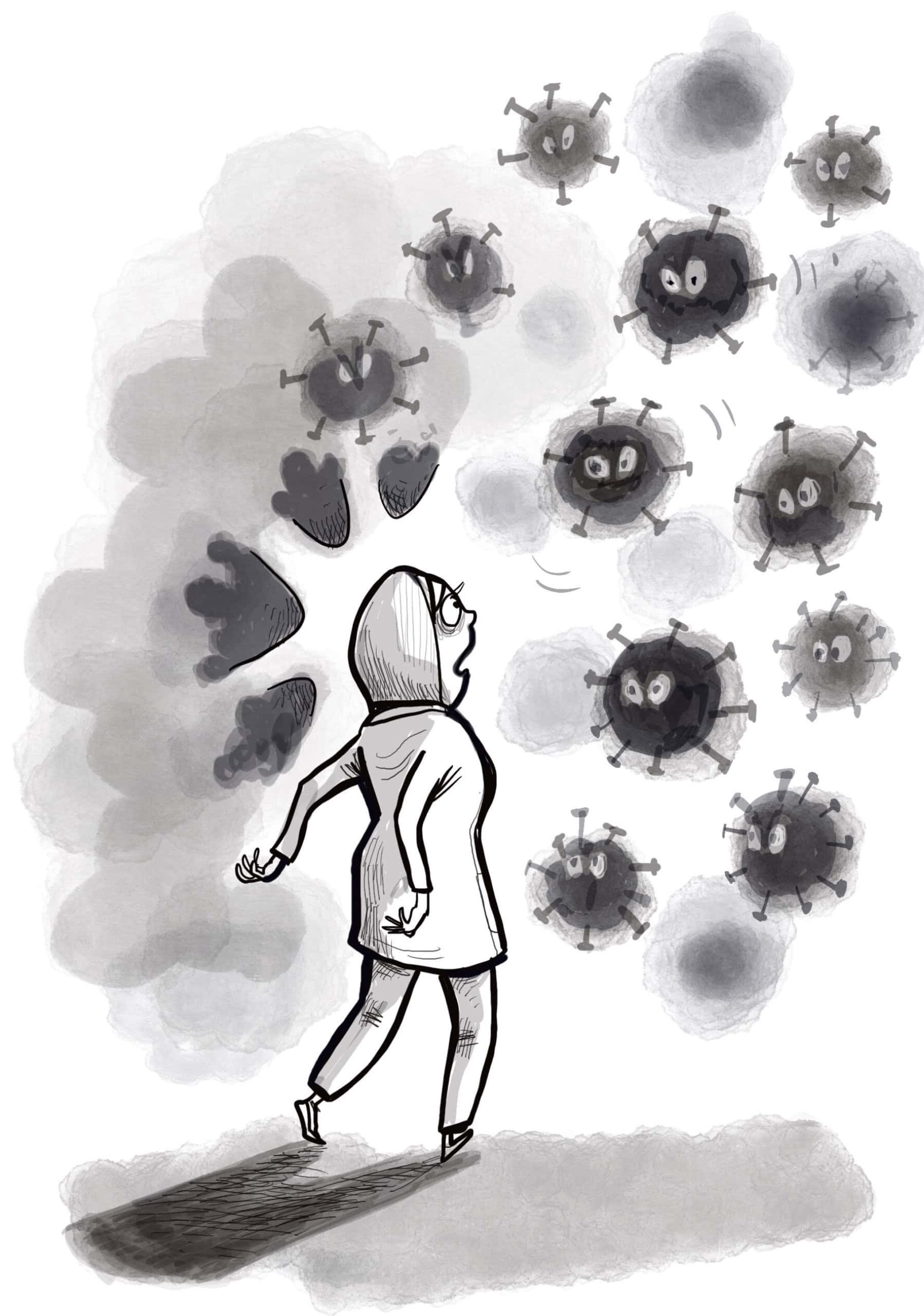
My two sons have asked me why I never seem to put them to sleep at night. “I miss you,” they said.
My work as a nurse in a public hospital is, however, both mentally and physically demanding. When I get home, I barely have time to cook, clean, and care for my kids. But if I don’t make time for this, I’d feel like a bad mom. Not gonna lie, life feels like a never-ending battle against time.
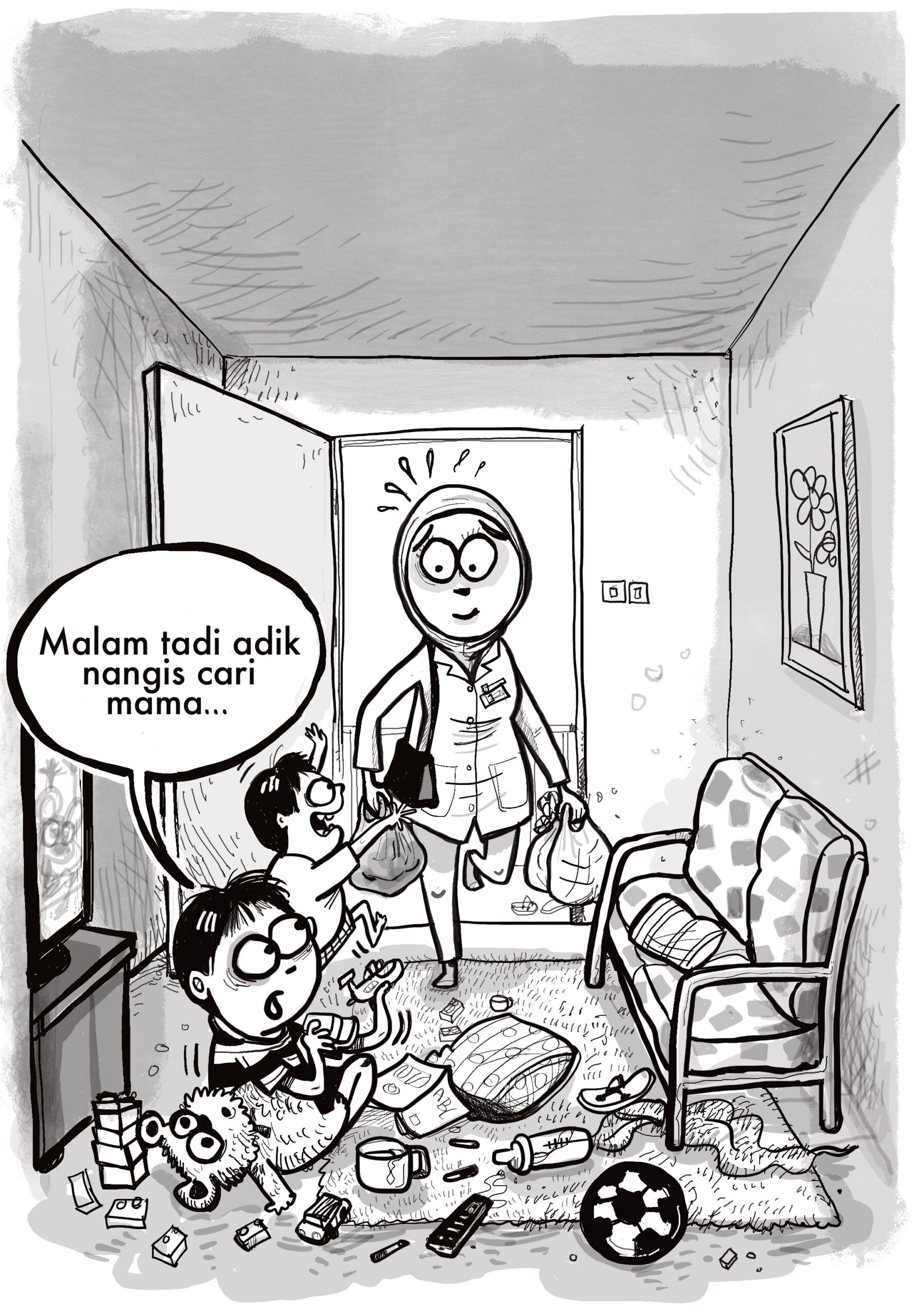
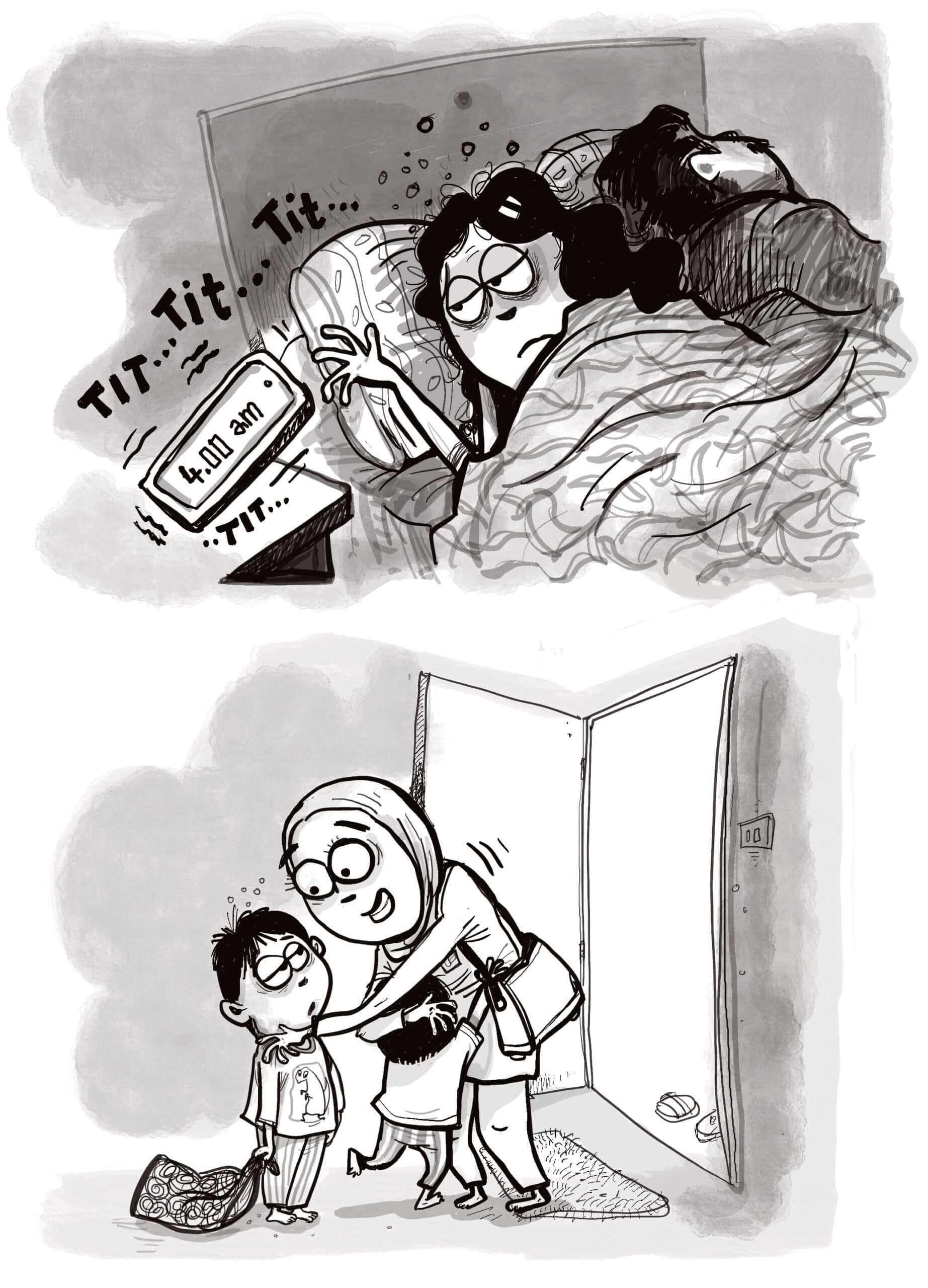
My alarm rings at 4am. I’m exhausted, but I’m up!
Every minute counts when you are juggling a full-time job and motherhood.
Also, I do feel good when taking care of other people, whether it’s a patient or my family.
The sense of purpose and pride in doing my job, the gratitude in the eyes of those under your care, the improvement and growth in their lives, well, all these get me out of bed in the morning.
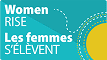
That is until the Covid-19 pandemic hit.

Suddenly, my sense of purpose transformed into fear.
My workload grew as terrifyingly as the infection rates and deaths.
The overwhelming in-flow of patients in critical states, the constantly shifting safety procedures and rules, the longer shifts, and the disrupted breaks – we were unprepared for the drastic increase in responsibilities and uncertainty.

We did our best, because we understood what was at stake—people’s lives, someone’s mother, someone’s child. This was, afterall, a health crisis!
So we hid our sweat, tears, and weary bodies in our personal protective equipment (PPE).
We buried our feelings so that we can work like machines.

Still, machines we were not.
Frustrations built up as we got more tired, which strained our communication as a team.
Fear gripped junior nurses who had to fill the staffing needs in the Intensive Care Unit even though they were undertrained and ill-equipped to handle complex cases.

Guilt also grew in me as patients and their loved ones begged me to let them see each other, but it was also my job to make sure everyone followed the strict safety protocols.
I understood the pain of their separation. Like the quarantined patients, I was also stuck in the hospital. Our shifts got longer and longer1. Our families could not reach us. The tsunami of work made it difficult to answer any calls or texts. There were several times when my husband tried to call me because he could not convince our son to eat, and he got angry that I did not call back for hours. I feel like a bad mum. I miss my family and worry for them too.
1 A national audit found that nurses in Intensive Care Units (ICU) often work more than 12 hours daily during the Covid-19 pandemic, and would be on double duty. In the RE:CARE study, nurses reported a 23.1% increase in working hours during the COVID-19 pandemic, compared to before the pandemic.

But there were lives to save. So we carried the pain of those under our care, while holding our own.
We managed emotions and demands—from family members who could not visit the patients; from our lonely and scared patients begging to see their families one last time. I helped elderly patients video call their family in their last moments. We listened to patients’ dying wishes—mindful of the promises we made to convey them to their families.
It’s hard to draw a boundary amidst the onslaught of needs. Our work and family lives bled into each other.
I remember my chat with Mala, a young cleaner who was cleaning the same ward I was working at that week. We had just finished our shifts and were cooling off after sweating profusely in our PPE the whole day.

We talked about not having seen the sun, and our sons, for days.
Mala told me that cleaners were also working longer hours due to the increase in patients. Often, if new patients come in just as she was about to go off shift, she was expected to keep working. There was no overtime pay, no bonus. Her husband bitterly questioned why she was coming home later, and sent her angry text messages to complain whenever their toddler cried and said things like, “Anak awak ni mesti nangis sbb u sayang hospital tu lebih drp dia2″.
2 Translates to “Your son must be crying because you love the hospital more than you love him.”

“It’s like we have to be superwomen,” Mala said while using a towel to dab her sweaty brows, or maybe her tears.
“We want to do our job well AND take care of our family. Now, it feels like I’m failing at both. Maybe I should do more.”
But how much more?
This question would not leave my mind for days after that. It swirled in my head as I struggled to turn heavy bedridden patients so that they can be cleaned; as I return home at midnight and see the overflowing laundry basket and greasy takeaway food containers on a sticky dining table; as I listened to a tearful colleague whose husband told her to quit her job to care for her mother-in-law suffering from long COVID complications.

Why are women expected to do more? Our jobs are demanding too. Yet housework and caregiving for children and elderly parents are still mainly seen as our duties, while no one bats an eye if our husbands put in only bare minimum effort.
Is it because caregiving is women’s responsibility alone? Or is my work ‘less important’ because I earn a smaller salary3 than my husband?
3 According to a news report, one nurse’s basic salary in Malaysia was less than RM3,000 after more than a decade of service. Most of the nurses involved in the RE:CARE study also reported salaries within the range of RM2,209 to RM4,580.

Why is my salary so low? I have been in this job for 15 years, after all.
If you ask me, I think it’s because people regard nursing as a ‘woman’s job’ – the perception is that much of it is merely caregiving, although we actually went through rigorous medical training.

Also, women are already paid less than men across many industries. Combine these two factors and it’s no surprise that nurses are undervalued.
The low pay, lack of status, and ‘women’s work’ stereotype do not only affect nurses. It is a headache for the whole healthcare system.

Nurses are the backbone of healthcare – we handle everything from diluting and administering medication to ensuring patient hygiene and preventing infection to crucial paperwork.
But Malaysia is losing nurses.

Just last year alone, I have seen about 30 colleagues leave Malaysia to work in other countries like Singapore or Saudi Arabia, where nurses are paid triple or more.
And not enough young people are joining nursing locally to replace the brain drain, especially since most men stay away from the profession. The lack of men is a problem. There are many parts of our job that require heavy-lifting, because we have to physically move patients.

There were a few times when I had to ask the hospital cleaners, also mostly women, to help me wrap up a dead body in the Covid-19 ward, even though it was not their job and it put them at risk.
Kak Gayatri, another cleaner whom I see often, told me that if they contracted Covid-19, they would have to be quarantined for 14 days and would receive no pay during their absence. I felt terrible, so I stopped asking them and tried to handle it myself.

Many of my female colleagues ended up having slip discs and other back issues, which forced them to take light duties or leave the profession entirely.
This makes the staffing shortage even worse. Patient treatments become slower; our work shifts get longer. And the more exhausted we are, the more we are prone to mistakes and injuries.
The cycle continues. Who suffers? All Malaysians.

But these are not new problems. The care economy in Malaysia is overwhelmingly made up by women4, who have long borne the brunt of caregiving duties at two fronts – paid ones at work and unpaid ones at home.
I, for instance, was already stretched thin even before the pandemic. But the weight of the Covid-19 health crisis made things worse, and made these problems clearer to me.
4 Women make up 96% of nurses in Malaysia, according to data from a 2019 report by the Ministry of Health.

It’s hard for me to get out of bed after COVID-19. It feels like I am set up to fail, both at work and at home.
But I get up anyway, because I am hopeful for change.
Some things are within my control. I started teaching my husband to cook healthy meals that our children like. He actually fell in love with cooking and started his own YouTube channel. I also no longer silently clean the house and dirty laundry, but told him that he has to do it if I am working the night shift. I also trained my sons to wash their own dishes and tidy up their own mess before bed.
Of course, sometimes they don’t do it perfectly. But I choose to let it go; it’s more important for me to have the time for rest than to have perfectly done chores.

But some changes are beyond my power. We need better policies to support and elevate the caregiving profession in terms of status and salaries, because Malaysia needs more care workers. More people valuing and participating in the care economy could mean better quality care for everyone.
I wish more men and women alike can experience the joy of providing good care. Yes, it is hard work. But caregiving, like life itself, feels easier and lighter when shared equally.